“Our Goal Should Be to Crush the Curve”
A doctor-scholar who studied the 1976 mishandling of swine flu says the president is wrongly choosing between saving lives and saving the economy.
Here’s what Harvey Fineberg thinks government officials should be doing…
We are in a desperate situation where the economy has tanked and hundreds to hundreds of thousands or more Americans’ lives are in jeopardy.
The choice is not one or the other.
The choice is what is the mix of policy and strategy and execution that optimizes the best outcome, given where we start today with both a serious pandemic and a fractured economy.
From an economic point of view, ironically, there is an optimal choice. There is a dominant choice, and that choice is based on experience in other countries that we can adapt — and based on the as-yet incomplete commitment to solve this problem.
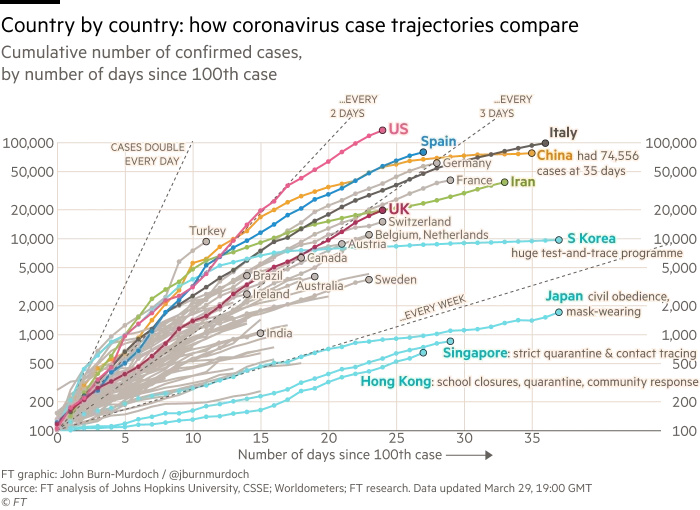
Our goal should not be to flatten the curve. Our goal should be to crush the curve.*
We should be mobilizing under the leadership of a supreme commander who has the full confidence of the president and can act with the full power and authority of the presidency, to mobilize every resource of the federal government, civilian and military, to win this war against the coronavirus. We should set a goal of achieving victory in 10 weeks. We should make this year’s D-Day victory over coronavirus day.
First, we need to have adequate numbers of tests available and distributed for diagnosis.
We do not have that in place, and it must be within two weeks.
Second, we need to provide protective personal equipment to every health professional who is going to be caring for patients.
We would not send soldiers into war without body armor. We should not ask our health professionals and attendants to serve without adequate protection.
Third, every citizen in the United States has a part to play. We should all be mobilized.
Everyone should be maintaining a physical distance. In public, everyone should now be wearing a surgical mask. Surgical masks should be delivered to every American household by the U.S. Postal Service, perhaps also mobilizing and utilizing the Amazons, Walmarts, Costcos, CVS, Walgreens and other major distributors.
All should be mobilized to get those surgical masks and hand cleaner in the hands of every American household.
The surgical masks do not prevent you from receiving the virus. But if everyone wears them, they will diminish the spread from those who are unknowingly infected to others.
Next, we need to test enough to be able to classify every American as documented infected, suspected infected, exposed or not yet known to be either exposed or infected.
Each of those classes of Americans needs to be treated appropriately.
Everyone who is infected or presumed infected — because the test, by the way, is not perfect — should be separated into dedicated clinical facilities. Serious cases and those at highest risk should be hospitalized.
Every convention center in every major American city should be converted into an infirmary where presumptive cases and documented cases with mild illness can be cared for and segregated, both from the general community and from other patients with emergent and urgent needs that are not infected.
Everyone who has been exposed to an infected person should be placed in quarantine.
All the hotels that are now empty in our cities could be mobilized with the staff retrained on appropriate sanitation procedures to be able to house, in comfort, dignity and appropriate care, those who need to remain in quarantine for a two week period of time, which would allow 99% of those who are going to develop symptoms to already have expressed symptoms.
If we take these steps and we simultaneously work on new treatments, a vaccine — which, by the way, will not come online in 10 weeks but will be available as a further deterrent after the acute victory — we can turn the tide and defeat coronavirus.
This is totally different from the response to the 1976 swine flu when no epidemic appeared. But this is the kind of radical approach that actually would bring together intelligent political decision making with expertise that can solve the problem from a scientific and public health point of view.
And by the way, if we do this, it is the best way to get the economy moving again. Because if we eliminate the threat of coronavirus in the space of 10 weeks, the economy can be sparked into action.
If we proceed in ways that are half-measures, incomplete approaches, gradual and not effective, we will persist with people falling ill, with people fearful, with workplaces disrupted, with an inability to get the economy humming again.